Cervical radiculopathy is caused by a pinched (or irritated) nerve in the neck. Physical therapists classify this condition as “neck pain with radiating pain” (1). Cervical radiculopathy can cause burning, numbness, tingling and weakness. The nerve irritation causes neck pain with radiating symptoms into the shoulder, upper back, arm, and hand.

Ever slept with your arm in a weird position? Or sat on your foot for a few minutes? That “pins-and-needles” sensation is similar to what cervical radiculopathy feels like. Except with a pinched nerve, symptoms linger.
Relevant Anatomy
The cervical spine consists of 7 vertebrae. C1 (at the top) supports your skull and C7 sits at the base of the neck. C7 or T1 (directly below C7) is the most prominent vertebra at the bottom of the cervical spine.
It’s pretty easy to feel on your neck, give it a try!

Each vertebra has a corresponding nerve root which exits above it. For example, the C7 nerve root exits above the C7 vertebra.
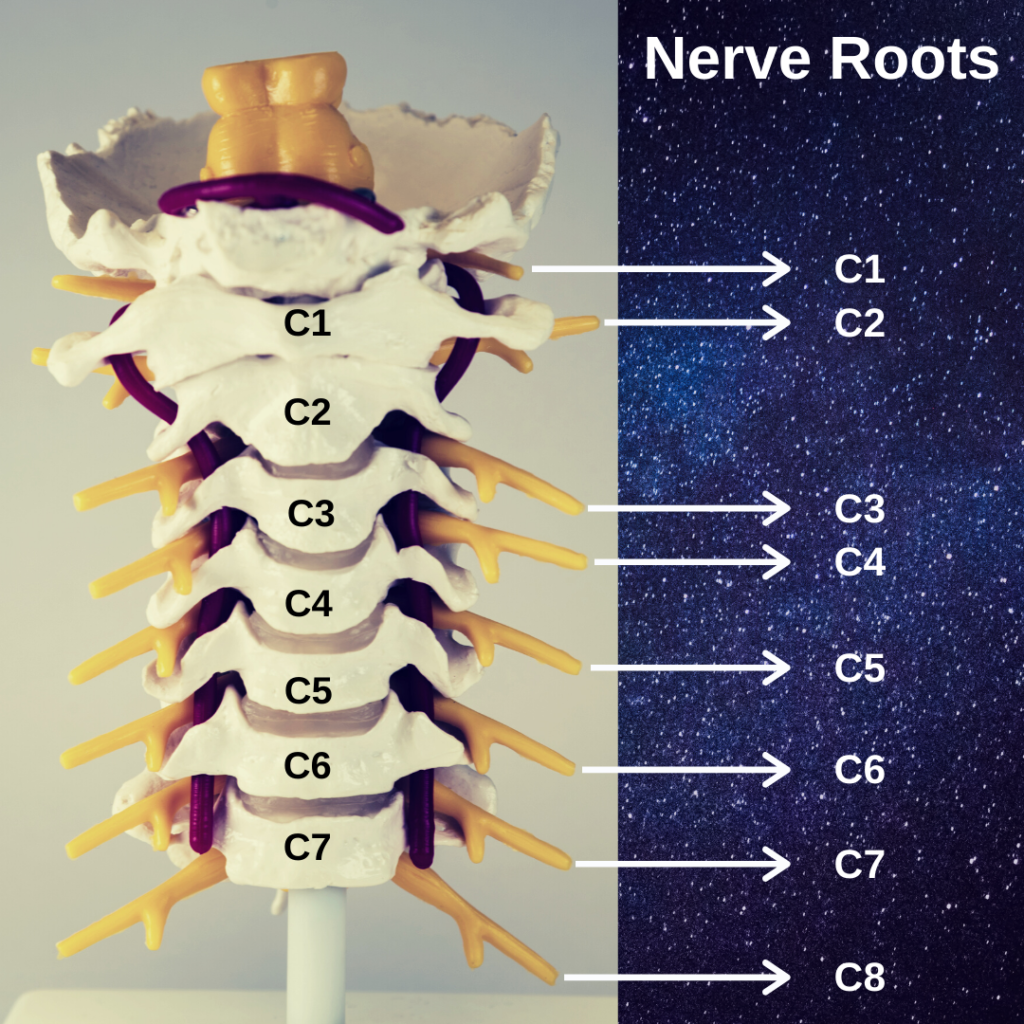
In a puzzling twist of anatomical nomenclature, there’s a C8 nerve root but not a C8 vertebra. The C8 nerve root simply exits below the C7 vertebra.
Nerves from the neck travel into the arms to provide sensation and strength. Cervical radiculopathy (irritation of a cervical nerve root) causes weakness and sensation changes in the shoulder, arm and hand.
How Common is Cervical Radiculopathy?
Cervical radiculopathy affects 1 to 2 in 1,000 people each year. Men get cervical radiculopathy almost twice as much as women. It affects adults in their 30s and 40s at the highest rates (2).
What are Risk Factors for Cervical Radiculopathy?
Cervical radiculopathy is most common in people who are white, smoke cigarettes or have a history of lumbar radiculopathy (2).

It often starts without a traumatic or inciting event. 30% of cases start during sitting, standing or walking (2).
What Causes Cervical Radiculopathy?
Several anatomical causes of cervical nerve root irritation have been proposed (2):
- a disc bulge protrudes into the nerve
- bone spurs push on the nerve
- loss of disc height narrows the nerve’s pathway
It’s important to remember that pain is complex and multi-factorial. It doesn’t always reflect tissue injury (3). Lifestyle and personal factors affect pain levels and recovery from cervical radiculopathy (4).
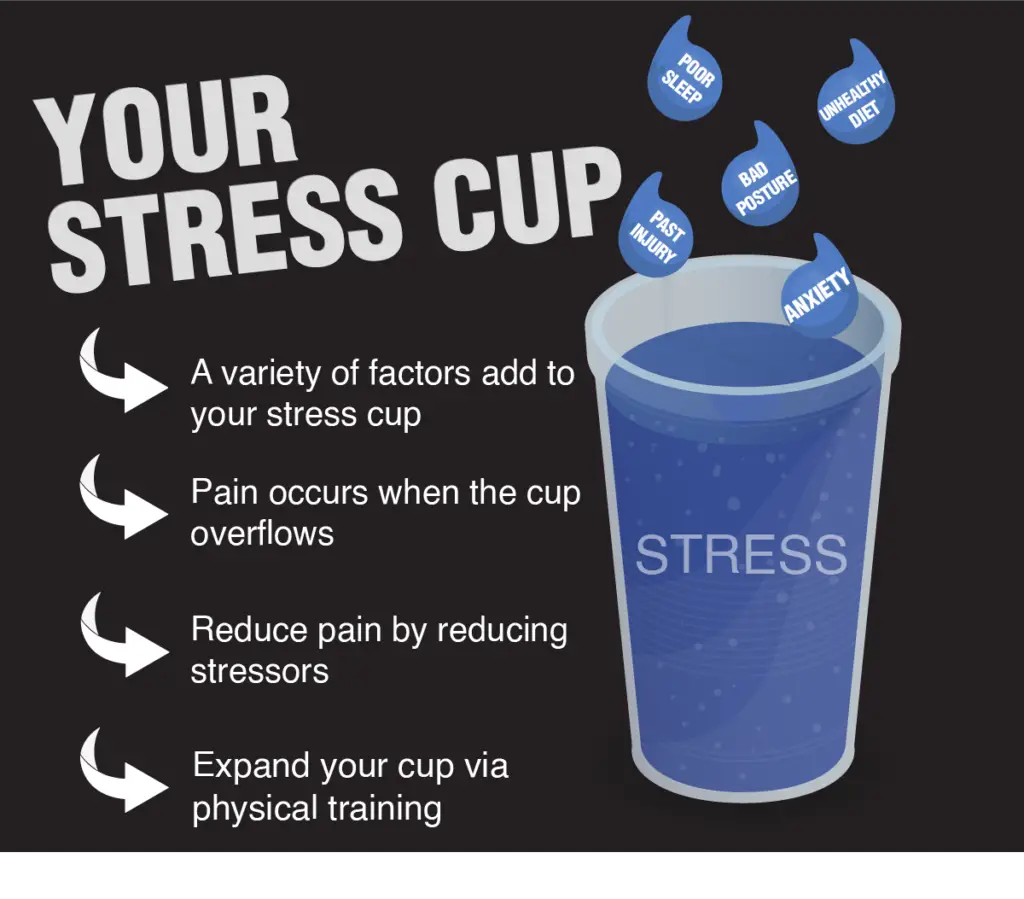
For example, patients who sleep well, stay active, eat healthy and manage their stress levels recover faster than those who don’t.
Expect a slower recovery if your 3 main food groups are beer, cake and cigarettes.
Does your nutrition need a tune-up? The Understanding Healthy Eating e-book is a great place to start.
If you’re not sleeping well, learn how to ease neck and shoulder pain at night.
Will I Need Surgery?
Probably not.
The prognosis for cervical radiculopathy is very good. Four years after symptoms start, 90% of patients are pain-free or have mild symptoms. Cervical radiculopathy rarely progresses and is usually self-limiting, meaning it eventually resolves by itself (2).
You’re probably thinking, “4 years is a long time! How about short term prognosis?”
Great question.
Even without treatment, most patients’ symptoms ease within 4-6 months. Pain reduction lasts for at least 2-3 years (2).
Physical therapy can help speed up the recovery process and alleviate symptoms (1). Keeping reading to learn the best treatments!
Neck surgery is typically a last resort if patients fail conservative treatments and symptoms don’t resolve in 6 months (2).
How is Cervical Radiculopathy Diagnosed?
Cervical radiculopathy is often diagnosed via the history provided by the patient (2). Common features include neck pain, pain in one arm, numbness, tingling, burning and weakness.
Physical examination also helps clinicians diagnose cervical radiculopathy. Muscle weakness, decreased sensation and diminished reflexes are common physical exam findings with cervical radiculopathy (2).
Physicians and physical therapists employ a cluster of four tests to confirm the diagnosis of cervical radiculopathy (5). The tests are illustrated below:




Positive findings for 3 or 4 test items help rule-in (confirm) the diagnosis of cervical radiculopathy. The Upper Limb Tension Test A (see above) is the best single test to rule out cervical radiculopathy (5).
Further testing is sometimes warranted. EMG testing can clarify the location and extent of nerve involvement. MRIs can identify soft tissue causes of nerve irritation, such as disc bulges (2).
Red Flags
As the name suggests, red flags are warning signs. Your PT looks for these during your examination.

Symptoms mimicking cervical radiculopathy can indicate something more serious may be going on. It’s important to get medical attention for red flag symptoms.
These are a few examples, not a comprehensive list:
- Crushing chest pain with radiating pain into the arm
- Numbness, tingling or weakness in both arms or legs
- Arm weakness with loss of balance, facial drooping or difficulty speaking
- Arm symptoms with changes in bowel or bladder function
Serious, life-threatening medical issues can cause symptoms in the neck. When in doubt, seek medical attention from a qualified healthcare provider who can assess your situation.
Your favorite online symptom checker doesn’t count!
Examples
Let’s get into specific examples of how cervical radiculopathy affects patients.
Cervical radiculopathy usually affects the C7 nerve root. C5, C6 and C8 involvement is less common (2,6). I’ll explain typical symptoms from irritation of each nerve root.
But first, I strongly caution you against diagnosing your own symptoms. Self-diagnosis is a tough task, even for highly trained medical professionals.
Just like you’d call an electrician to handle a complex rewiring project, talk with your PT or physician if you think you have cervical radiculopathy. Trying to DIY can fry your nerves and leave you in a worse predicament.
C5 Radiculopathy
As you can see below, C5 nerve root irritation creates numbness, tingling and pain in the front of the shoulder and elbow.
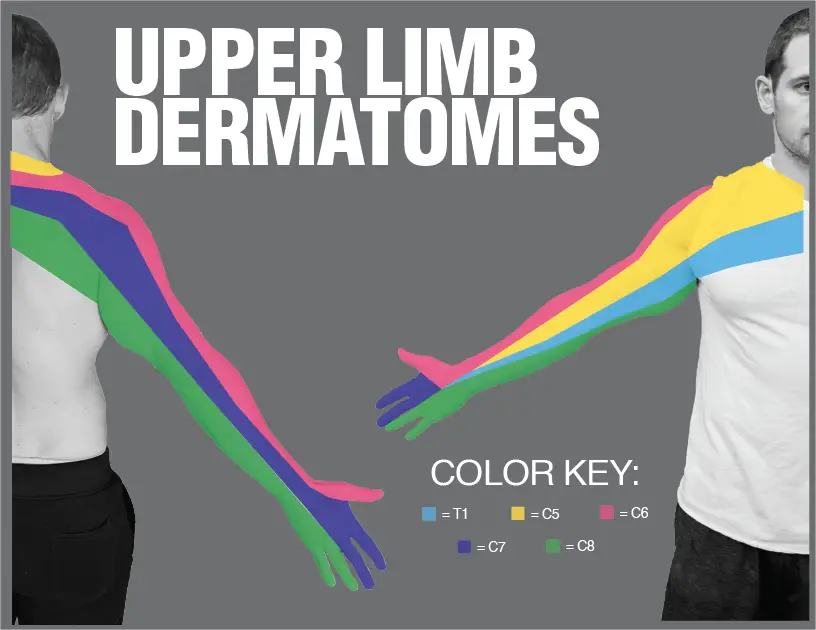
C5 innervates (i.e. provides nerve signals to) the deltoids and all 4 rotator cuff muscles–the teres minor, infraspinatus, supraspinatus and subscapularis. C5 radiculopathy can cause shoulder weakness and difficulty reaching overhead.
C6 Radiculopathy
C6 nerve irritation causes pain, numbness and tingling along the lateral shoulder, elbow and into the thumb. C6 supplies the muscles that flex the elbow, so weakness with pulling and lifting (think of a biceps curl) is typical of C6 radiculopathy.
C7 Radiculopathy
C7 radiculopathy accounts for 81% of cervical radiculopathies (6). In the clinic, weakness with resisted elbow extension is a hallmark of C7 irritation.
C7 nerve root involvement can cause symptoms along the posterior shoulder, elbow and hand into the index and middle fingers.
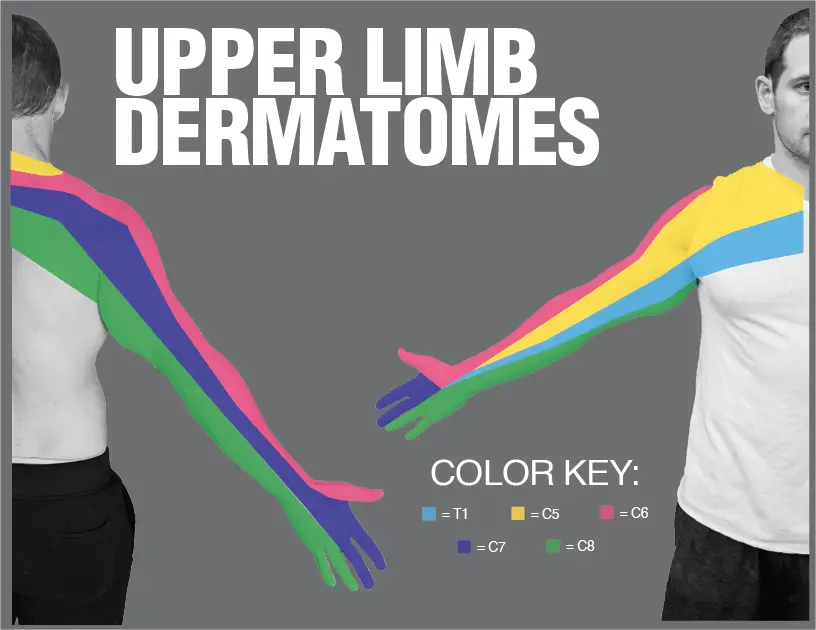
C7 supplies elbow extensors, such as the triceps brachii. Patients with C7 radiculopathy experience weakness with push-ups, bench press and triceps exercises.
C8 Radiculopathy
C8 irritation causes sensation changes along the posterior shoulder and upper arm. Symptoms may radiate into the back of the elbow and all the way into the ring and pinky fingers.
C8 provides motor input (strength) to many of the hand muscles. C8 radiculopathy can cause difficulty gripping, manipulating objects and opening tightly-sealed jars.
C8 represents 4-12% of cervical radiculopathies (6). Hand weakness and changes in sensation can originate from many sources besides C8 radiculopathy. Ulnar nerve irritation and carpal tunnel syndrome also cause hand symptoms.
If you have questions about your symptoms, get evaluated by a qualified healthcare professional.
Treatments
There are a plethora of treatments for cervical radiculopathy. We’ll cover several conservative options. Time and conservative treatment resolve most cases of cervical radiculopathy (2). More aggressive management, like injections and surgery, can help in severe cases.
Cervical Retractions
Sometimes called chin tucks, cervical retractions are my go-to exercises for cervical radiculopathy. Retractions can rapidly ease or resolve symptoms. And patients can do them on their own at work or at home.
I don’t want patients to rely on me long-term; I’d rather give them tools to manage their symptoms independently. This exercise helps.
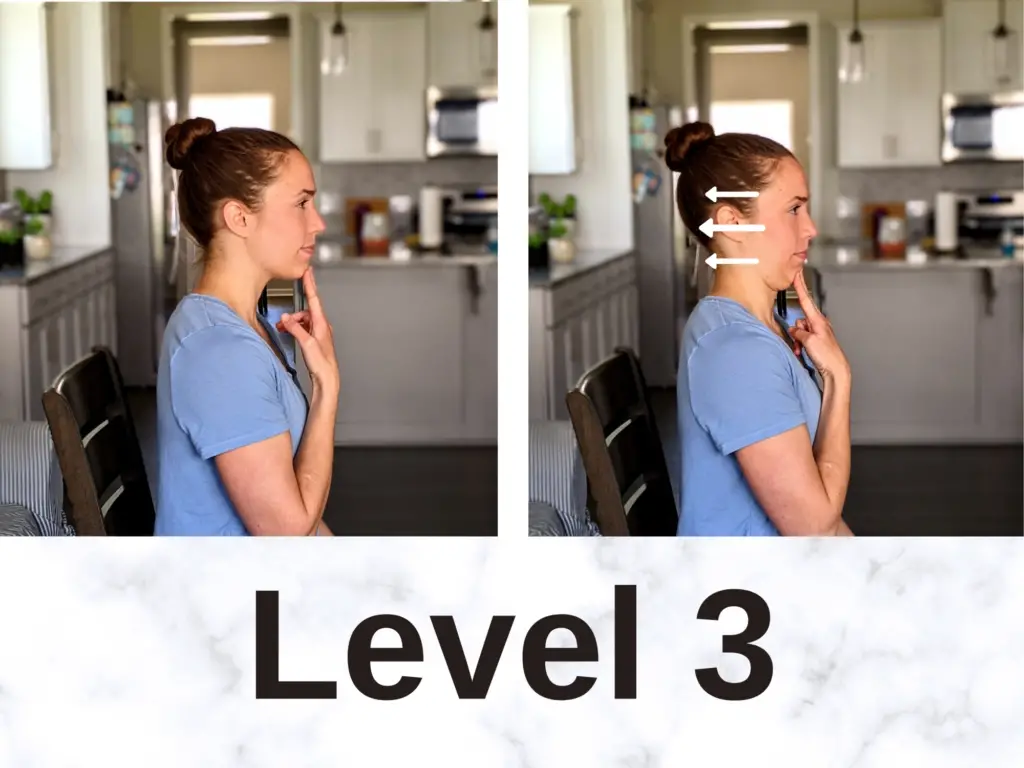
There 3 variations of chin tucks illustrated below:
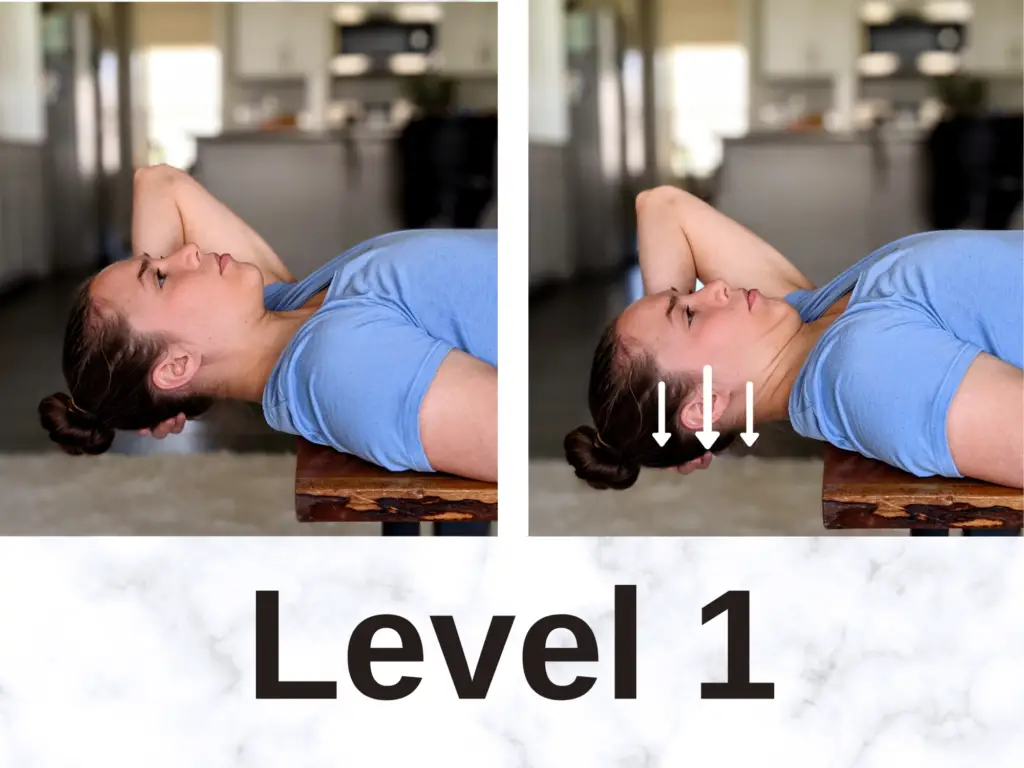
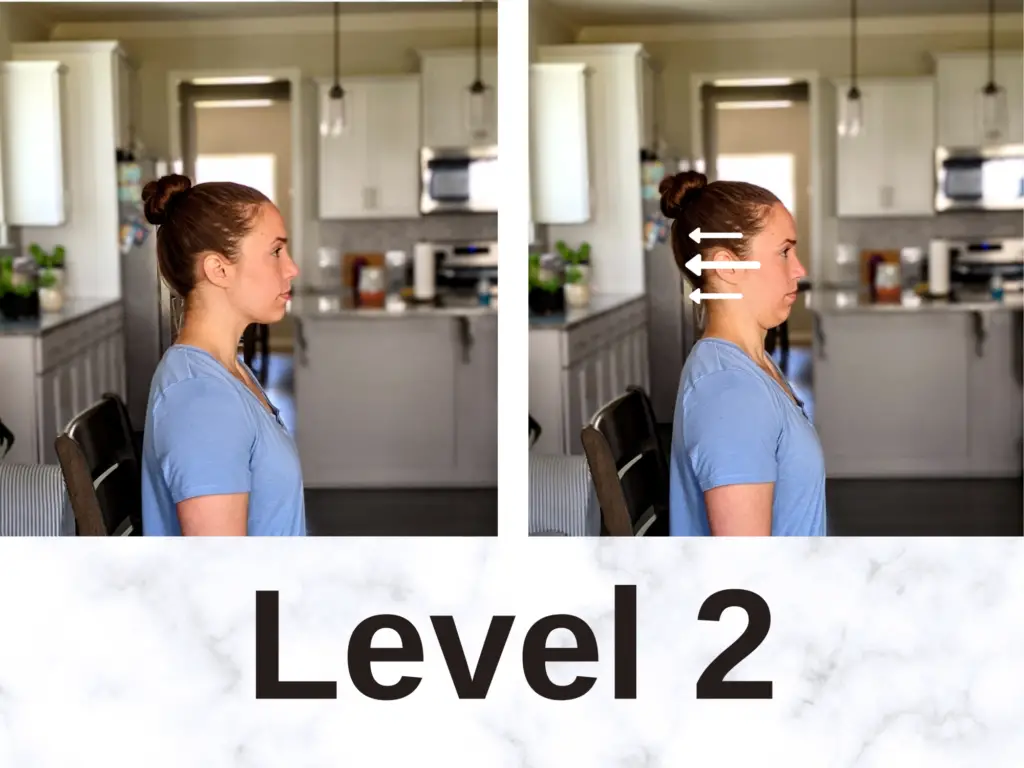
Level 1 typically works best for highly irritable symptoms. If the other variations aggravate arm symptoms or send symptoms towards the hand, Level 1 can help.
Level 2 works for many people with cervical radiculopathy and Level 3 helps once symptoms have calmed down a bit.
It’s easy to tell whether chin tucks are helping. Positive signs include:
- pain location moving up the arm towards the spine
- less pain afterwards
- increased arm strength
- increased neck range of motion.
“Centralization” describes pain that moves towards the spine. For example, pain leaves the hand and settles in the upper arm. Patients who demonstrate centralization feel better faster (7).
Patients usually benefit from one set of 5-15 repetitions every 1-2 hours for a total of 40-60 repetitions per day.
Chin tucks are thought to improve disc hydration and reduce irritation at the affected nerve. This exercise is a staple in the McKenzie Method of diagnosis and treatment. The McKenzie Method uses repeated motions and changes in symptoms to assess an exercise’s effectiveness.
Check out this book to Treat Your Own Neck with the McKenzie approach.
Cervical Traction
Cervical traction is a controversial treatment. Some research indicates it relieves cervical radiculopathy, while other studies show it’s no more effective than a placebo (2,8).
One study (9) identified 5 characteristics of patients who respond well to cervical traction:
- Age over 54 years old
- Relief with neck distraction test
- Positive Upper Limb Tension Test A (see Diagnosis section above)
- Peripheralization of arm symptoms with C4-C7 mobility testing (symptoms move further down the arm, away from the neck)
- Positive Shoulder Abduction Test (palm placed on top of head, positive if arm pain reduces)
Current guidelines cautiously recommend cervical traction alongside manual therapy and exercise-based treatments for cervical radiculopathy (1).
In my experience, traction often relieves radiculopathy symptoms, but the relief isn’t always long-term. I use cervical traction occasionally if chin tucks aggravate my patient’s arm symptoms.
Most patients respond positively to chin tucks which can be performed independently. Cervical traction is challenging to do without assistance.
If patients benefit from cervical traction in the clinic, an at-home cervical traction device can give them more frequent pain-relief. I like the portable option which provides a gentle traction force to the neck, relieving pain:
Nerve Mobilization
Treatment guidelines support nerve mobilization for cervical radiculopathy (1,10). Nerve mobilization reduces nerve swelling and hypersensitivity to promote nerve healing (10).
There are two types of nerve mobilization exercises.
Nerve “sliders” floss the nerve back and forth without stretching the nerve. Imagine flossing your teeth. The floss slides side to side without stretching. Nerve sliders are like flossing.
When performed correctly, the patient feels nothing–no stretching, pain, or changes in symptoms during the exercise. Nerve sliders work best when the nerve is easily irritated, like the llama that kicked me in the thigh when I was 6.


Nerve “tensioners” gently stretch the affected nerve. They work best when the nerve is mildly irritable. Think of lightly stretching a rubber band from both ends. Tensioners are more aggressive than sliders. They can aggravate arms symptoms if done too aggressively. This isn’t a “no pain, no gain” situation.
Symptoms shouldn’t worsen after performing nerve glides. Further irritating the already-grumpy nerve isn’t beneficial.
Would you smash your thumb with a hammer a second time after missing the nail once? Same principle. Don’t go crazy with nerve tensioners.
Two sets of 10-15 repetitions per day is a reasonable prescription for nerve glides.
Thoracic Spine Mobilization
A stiff thoracic spine increases motion demands at the neck. Guidelines recommend hands-on thoracic spine treatment via manipulation or mobilization (1). Thoracic mobility exercises can help, too.
Think of the neck and thoracic vertebrae like a team of office workers. There are 7 in the neck and 12 in the thoracic spine. If 5 “workers” in the thoracic spine decide to slack off, the other workers have to do more work. Eventually, the overworked employees get upset!
Mobilizing a stiff thoracic spine puts the lazy workers back to work and spreads out the workload. Increasing joint motion in the thoracic spine can help alleviate neck pain.
Open Books are a great exercise to mobilize the thoracic spine:

Cervical Spine Mobilization
Manual therapy treatments for the neck are recommended for cervical radiculopathy in combination with other treatments (1,8). Mobilizing stiff joints in the cervical spine can reduce pain and motion demands at the involved region.
Cervical manipulation is a controversial treatment. Guidelines support its use for cervical radiculopathy (1). However, cervical manipulation has been linked to rare, but serious adverse events (2). For this reason, some clinicians opt for alternative treatment options.
Neck Strengthening
Deep neck flexors are the “abs” of the neck. These small muscles near the front of the throat help stabilize your neck and hold your head in neutral posture. Neck strengthening, and getting the deep neck flexors “swole,” helps with cervical radiculopathy (1,2,8)
Neck strengthening isn’t the best stand-alone treatment for cervical radiculopathy; it works best in combination with other treatments (1,2,8).

In the picture, I’m palpating the sternocleidomastoid (SCM) muscle, a powerful neck flexor. This exercise targets the smaller deep neck flexor muscles. The SCM will take over the exercise if the chin tuck is too forceful. Palpating the SCM helps monitor this muscle to make sure it’s staying relaxed.
Upper Back Strengthening
Like neck strengthening, this isn’t the #1 treatment to relieve cervical radiculopathy. But strengthening it’s often part of a successful treatment program.
These muscles also help support the neck and contribute to upright sitting and standing posture. Modified Superman’s strengthen the upper back:

Start lying on your stomach like a beached seal. Squeeze your shoulder blades down and back and raise your chest off the floor. Hold 5 seconds. Relax.
It’s important to keep a comfortable neck position during this exercise. Neutral neck position, looking at the floor under your face, is ideal.
Normal Activities
Guidelines encourage patients to continue their normal work and exercise activities as much as possible when recovering from cervical radiculopathy (1).
If sitting aggravates your symptoms, check out my post on 5 Ways to Sit With Less Pain
And be sure to read about how you can sleep with less neck pain.
Final Thoughts
Whew, that’s a lot to digest!
Cervical radiculopathy can be concerning diagnosis. It’s strange to have arm and hand pain coming from a different location! Fortunately, surgery is rarely needed and exercise-based treatments usually help.
Thanks for reading, comment below if you have questions or thoughts on cervical radiculopathy!
This information is intended for your education. It’s not medical advice. If you’re dealing with cervical radiculopathy, please consult a medical doctor or physical therapist.
For more evidence-based insights you won’t find anywhere else, join the free Facts & Physio Newsletter. Plus, get The Recovery Checklist when you sign up.


2 thoughts on “The Authoritative Guide to Cervical Radiculopathy (and 8 Effective Treatments)”
Thank you so much for this really detailed information. I have been suffering for 5 years now. Thought I never have tried the flossing exercises. That’s why I’m here , well that and along with more information to help me learn to beat this situation once and for all. That’s the hope and that’s definitely the game plan. Unfortunately I’m having issues on both sides (bone spurs on c-6 & c-7) and that’s not good. But I’m no quitter and have been working on improving my posture for the past year. If there is a way I have the will. This has been a challenging time in my life. And unfortunately this covid thing happened when I started my physical therapy. As I read somewhere before….Don’t let your spine get on your nerves. lol. Again thank you for doing what you do to help others!
Danny,
So glad you found the information helpful! You have a great attitude and I wish you the very best with your recovery