Shoulder impingement causes misery for many. Daily tasks like reaching to top shelf are excruciating. It’s even hard to sleep!

But there’s good news: conservative treatment, like physical therapy and doing the right exercises, can relieve pain and restore full shoulder function (1).
What is Shoulder Impingement?
Shoulder impingement occurs when “soft tissues become painfully entrapped in the area of the shoulder joint” (1). It’s most common with reaching overhead, behind your back, or across your body and down (like starting a lawnmower with a pull cord).
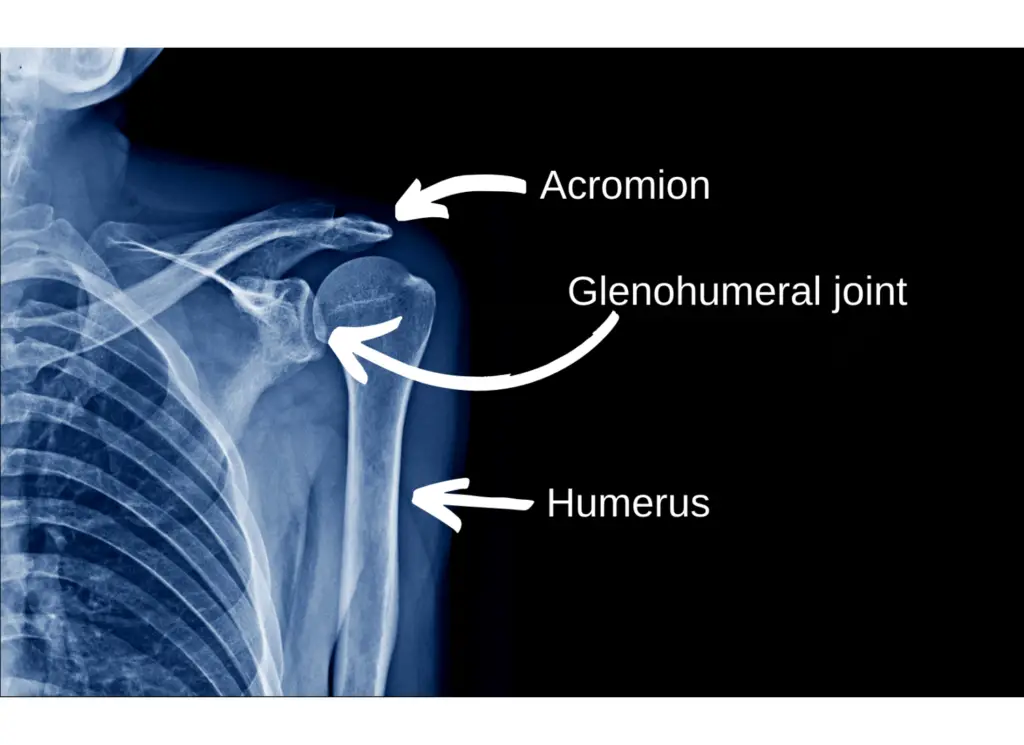
Most shoulder impingement occurs underneath the acromion process. The acromion is a bony prominence at the front of your shoulder, next to your collar bone.
See if you can feel the acromion process on your shoulder:

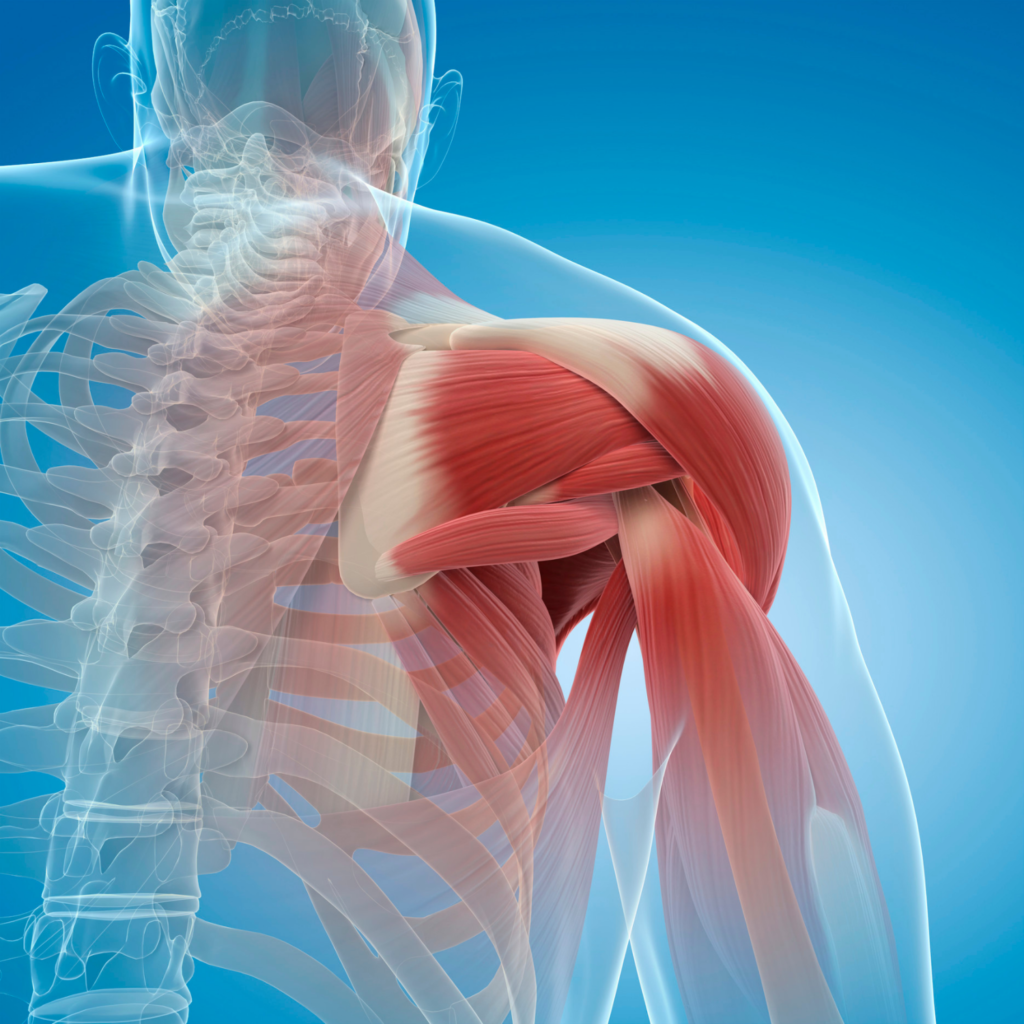
As we reach overhead, the humerus (upper arm bone) elevates, narrowing the space under the acromion. The supraspinatus muscle and subacromial bursa (bursa = fluid-filled sac) sit between the acromion and the humerus. With impingement, the muscle and bursa get pinched between the humerus and acromion.
The supraspinatus muscle (shown below) travels under the acromion and attaches to the humerus
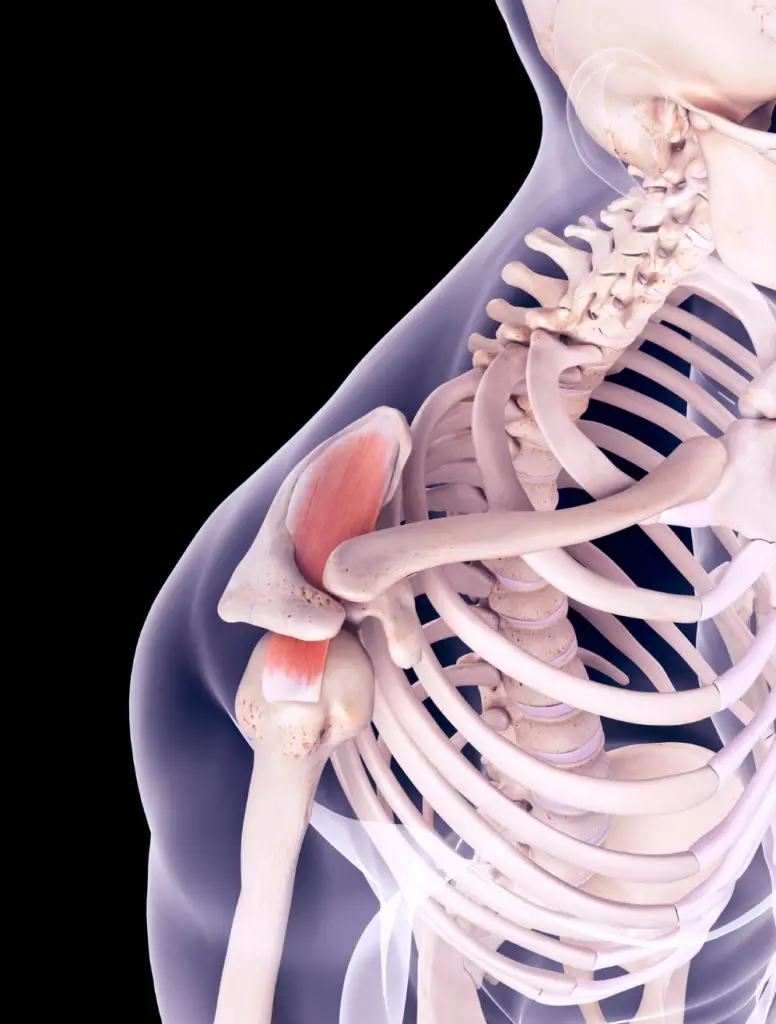
With enough irritation, the supraspinatus and subacromial bursa start hurting with overhead arm movements. Pain is felt on the front or outside of the shoulder.
Who Gets Shoulder Impingement?
Shoulder pain affects up to 30% of adults each month. Impingement syndrome is a frequent cause of shoulder pain. It’s most common from ages 50 to 60 (1).
How is Shoulder Impingement Diagnosed?
Physical therapists and physicians often use a 3-test cluster to test for shoulder impingement:
The Neer Test

The patient reaches overhead with thumb down. The clinician applies overpressure at end range of motion. Pain reproduction indicates a positive test.
Hawkins-Kennedy Test

The clinician internally rotates the shoulder and applies overpressure at end range of motion. The test is positive with pain reproduction.
Painful Arc Test

The patient lifts her arm into abduction all the way overhead. A positive test occurs when pain is recreated through the middle of the motion.
None of these tests is great in isolation, but combining them improves diagnostic accuracy (2). Even so, the 3-test cluster isn’t perfect.
X-rays rule-out bony injuries like fractures. But they don’t show soft tissues like muscles, tendons and ligaments. X-rays don’t show shoulder impingement.

MRIs show the soft tissues in the shoulder. However, abnormal imaging findings like a rotator cuff tear, bone spurs and arthritis don’t correlate well to shoulder pain–an MRI scan of the painful side can look the same as the MRI of the other shoulder! (3)
In short, diagnosis is tricky.
A Little Controversy
Research shows that physical therapy is a solid treatment for shoulder impingement syndrome (1,4). It works as well as surgery without the elevated costs and risks (4).
Plus, physical tests and imaging options don’t diagnose shoulder impingement well. And experts dispute the cause of impingement syndrome (4).
For these reasons, some experts question whether impingement is a valid concept or an accurate diagnosis. Several even advocate changing the term “impingement syndrome” to a generic term like “subacromial pain syndrome” (i.e. pain under the acromion).
What Causes Shoulder Impingement?
Shoulder pain is complex. It’s rarely due to a single cause. A confluence of factors contribute to shoulder pain. Postures, tissue status, loading, stress levels, sleep and nutrition all play a role in shoulder pain.
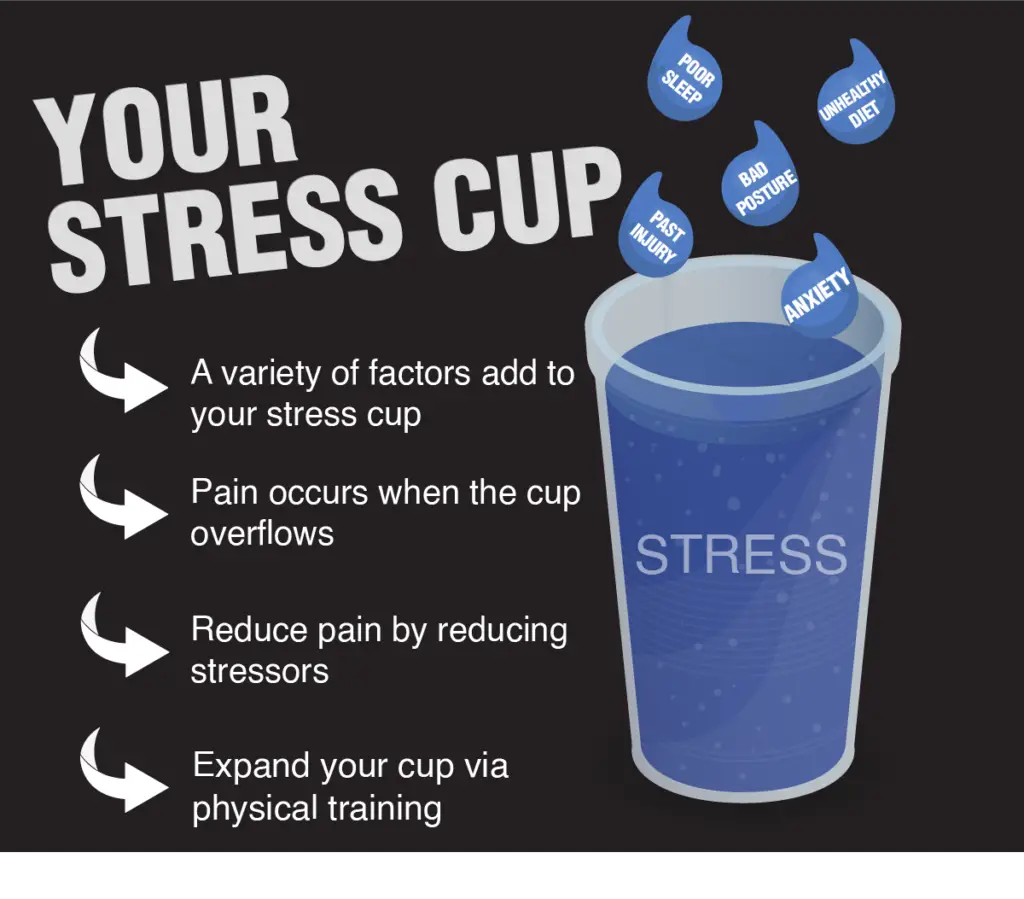
Taking care of these factors–having good posture, managing stress and sleeping well–are key to pain management and minimizing recovery time.
If shoulder pain hampers your sleep, read my strategies to ease shoulder pain at night.
Physical factors play a role in shoulder impingement, too. They can be remedied through exercise and working with a skilled physical therapist.
The 11 Best Shoulder Impingement Exercises
These exercises address common culprits in shoulder impingement. However, they may not be appropriate for everyone. If you’re dealing with shoulder pain, consult with a local physical therapist or physician to figure out the best approach for you.
The most important exercise for treating shoulder pain is…
1) Chin Tucks
Referred pain from the neck often produces shoulder impingement symptoms which resolve after treating the neck (5). Physical therapists learn to screen the neck before treating the shoulder joints.
I’ve worked with countless patients whose impingement symptoms disappear after a 30-second neck exercise. Patients think it’s magic.
In my experience, neck exercises immediately improve shoulder symptoms about half the time. A recent study corroborates this finding (6).
When a patient has shoulder pain, I always assess the neck. I use chin tucks (also called cervical retractions) to screen the neck:

Here’s how I structure the assessment: First, I establish a painful baseline motion, like reaching the arm overhead. Next, the patient does 10-15 chin tucks. Then we retest the shoulder baseline.
A significant improvement tells me the neck is contributing to the shoulder pain. Treatment starts at the neck.
Screening the neck is a critical first step for treating shoulder pain!
Rotator Cuff Strength
The rotator cuff consists of 4 muscles. This group of muscles stabilizes the glenohumeral joint, where the head of the humerus (upper arm) meets the glenoid cavity (shoulder blade).
The glenohumeral joint is the most mobile joint in the body. It’s a ball and socket joint. But it’s more like a golf ball sitting on a tee–big ball, small socket. Plenty of mobility but not much stability.
The rotator cuff muscles stabilize the glenohumeral joint. Weakness of these muscles increases the risk of shoulder impingement and pain.
2) Isometrics
Isometrics are a great option with irritable shoulder pain. Plus, isometrics have a pain-relieving effect for tendon pain (7).
Internal rotation and external rotation shoulder isometrics require nothing more than a doorway and towel:
I caution patients to avoid pushing through pain. Sets and reps depend on shoulder irritability. 2 sets of 10-15 reps, holding 5-10 seconds each is usually tolerable.
3) Scaption
These exercises simulate the initial part of reaching overhead. They are called scaption because they’re performed in the plane of the scapula (shoulder blade), 30° in front of sideways.
Lifting the arm in this plane allows plenty of bony clearance between the humerus and acromion to limit shoulder discomfort. Keep the thumb up to put the shoulder in a neutral position. Complete the exercise in a pain-free range of motion.

I instruct patients to lift the arm to shoulder height, but as rehab progresses, arm elevation can increase. Patients can do this exercise with or without weights.
Start with light weights since the hand is so far away from the body; the lever arm is extremely long which means the muscles have to generate a lot of torque to lift even small weights. (I apologize if this dredges up painful memories of physics class)
If you don’t have access to small weights, a water bottle or can of baked beans works just fine.
4) Sidelying External Rotation
This exercise beefs up the posterior rotator cuff–the infraspinatus, teres minor and supraspinatus–and it’s easy to progress. Progressive overload is key to getting stronger–gradually increasing repetitions and weight over time is a simple way to build strength.


Use a towel under the armpit to increase blood flow (8) and muscle activation (9) of the rotator cuff.
Thoracic Mobility
A mobile thoracic spine makes it easier to reach the cookie jar on top of the fridge. Just make sure Mom isn’t looking!
This is what normal thoracic mobility looks like:

On the other hand, thoracic spine stiffness makes the shoulder joint work harder and predisposes us to shoulder impingement:

Improving upper back mobility treats shoulder impingement by reducing the stresses on the shoulder.
Modern life puts us in a flexed position with our shoulders forward and upper back rounded. Especially if our work station isn’t optimal and we sit with poor posture. If that’s you, check out my guide on 5 Ways to Sit With Less Pain
5) Foam Roll Thoracic Extensions
Thoracic extensions move us in the opposite direction and mobilize the thoracic spine. As a bonus, they feel great!

“Knobby” foam rollers don’t feel as comfortable for thoracic extensions. This one will do the trick.
6) Open Books
These exercises improve the extension and rotation of the thoracic spine. Those motions help us throw a ball, swing a golf club, reach a high cabinet or grab the last package of toilet paper off the top shelf.

Shoulder Blade Stabilization
About 33% of our overhead shoulder motion comes from the shoulder blade (scapula) rotating upwards. If the surrounding muscles aren’t functioning properly, shoulder impingement is more likely (10).
These exercises optimize shoulder blade function.
7) Serratus Anterior Punches
The serratus anterior originates from the side of the ribcage and attaches on the inside of the shoulder blade. It stabilizes the shoulder blade and is known as the boxer’s muscle:

To perform this exercise, lie on your back with the arm straight. Punch the arm up towards the ceiling. Then return to your starting position. It’s a small movement.

8) Prone T’s
Prone T’s can be done with or without weight. They target the middle portion of the trapezius muscle (below):

Keep the arm in a thumbs-up position.


9) Prone Y’s
Perform these just like prone T’s, the only difference is the angle of motion. Prone Y’s target the lower trapezius muscle.


To make these tougher, grab your light weights or your can of baked beans!
Prehab
Four years ago my shoulder started hurting. It felt worse when I did overhead press and bench press. The pain forced me to stop lifting. I tried to push through the pain in the gym, but my shoulder just hurt more.

I was miserable.
It took patience and discipline to take time off from upper body strength training. But my shoulder felt better after a few weeks of rest, NSAIDs and gentle exercise.
I use the following exercises to keep my shoulders strong and happy, even with heavy bench pressing several times a week, and occasional not-so-heavy overhead pressing.
Since hurting my shoulder, I’ve bench pressed 360lbs, and my best overhead press is, well, still pretty weak.
Give these a try as part of your upper body workout!
10) Bilateral Shoulder External Rotation
Keep the elbows pinned to the side and bent to 90 degrees as you pull outward on the resistance band


This exercise strengthens the posterior rotator cuff muscles (supraspinatus, teres minor, infraspinatus) and the scapular retractors (rhomboids, middle trapezius).
11) Band Pull-Aparts
Last but not least, band pull-aparts will strengthen your upper back and improve your shoulder blade control. They’re my go-to exercise before a bench press workout.


I use a light resistance band for the prehab exercises, working in the 10-20 repetition range. I like the versatility of closed-loop band, like these.
Final Thoughts
If you’re dealing with shoulder pain, it’s a good idea to see a physical therapist. PTs are trained to assess your shoulder and prescribe the proper treatment for your specific situation.
Your physical therapist can provide manual therapy, patient education, and guidance on the best stretches and strength exercises for your shoulder.
Have you dealt with shoulder impingement? Let me know in the comments below!
For more evidence-based insights you won’t find anywhere else, join the free Facts & Physio Newsletter. Plus, get The Recovery Checklist when you sign up.


6 thoughts on “How to Relieve Shoulder Impingement (11 Physical Therapy Exercises)”
Great article. I did the chin tucks and already some significant relief!!!!! I’m going work on the rest of the exercises as well.
Glad to hear it, hope you make a quick recovery!
Hi Dr. Forsythe. I did all your exercises plus I watched a few YouTube videos about the upper trap and the levator scapulae. It’s been about 4 days and I’m still having sharp pain near my collarbone. My PT can’t get me until a month from now and I was wondering if you could help specifically with pain on collarbone. It hurts the most at the top of a shrug and when I roll my shoulder forward and backwards. Either way, thank you for this digital guide!
Hey Lauren,
It sounds like the traps might be involved, but it’s hard to say for sure just from the symptom location. I do offer virtual consults, so if you want me to take a closer look and give you targeted exercises to address this issue until you can get in to your PT, that’s an option. Here’s the virtual consult info if you’re interested: https://factsandphysio.com/virtual-consult-application/
Thanks for the comment,
-Jacob
Have pain about 4 inches or so down from top of shoulder, in the back, between shoulder blade and spine- When i move just right, feels like a rubber band snapping (like if you snapped the band on your arm or soemthing)- I also get small knots there that make it very painful for several days to 2 weeks sometimes in the same general area- they can move around. I have a percussion massager that helps some, but it takes a long time for that pain to stop- The snapping pain though usually only lasts a day or 2. What i9s causing that snapping sensation? It will cause pain right therefor a little while- I do have bad posture, and know that is contributing- but when the knots hit wow- can’t hold my head up for long without havign to sit and lay head rest on back of couch or chair- that pain lasts for a week or more- off and on in severity of course-
Hey Bob,
Thanks for the comment. It’s tough to say what is causing this sensation without a physical exam. It sounds like your symptoms are in the neck or thoracic spine area more so than your shoulder – classic shoulder impingement is on the front/outside of the shoulder. Check out these articles and let me know what you think:
https://factsandphysio.com/mid-back-pain-exercises/
https://factsandphysio.com/tight-neck-muscles/
-Jacob