Ulnar nerve entrapment causes pain, numbness, and tingling in the arm and hand.

The ulnar nerve is one of three main nerves in the upper limbs, along with the median nerve and the radial nerve.
Ulnar nerve irritation occurs at the neck, at the wrist, or (most commonly) at the inside of the elbow. Ulnar nerve compression at the elbow is called cubital tunnel syndrome.
Conservative treatments relieve ulnar nerve entrapment for 50% of people with mild to moderate symptoms. And there’s good news for those who don’t recover with conservative treatment; surgical success rates are high.
Ulnar Nerve Anatomy
The ulnar nerve runs from the neck, down the inside of the arm, to the pinky side of the wrist. It supplies strength to several wrist flexors in the forearm and many intrinsic hand muscles. It also provides sensation to the pinky finger and half of the ring finger.
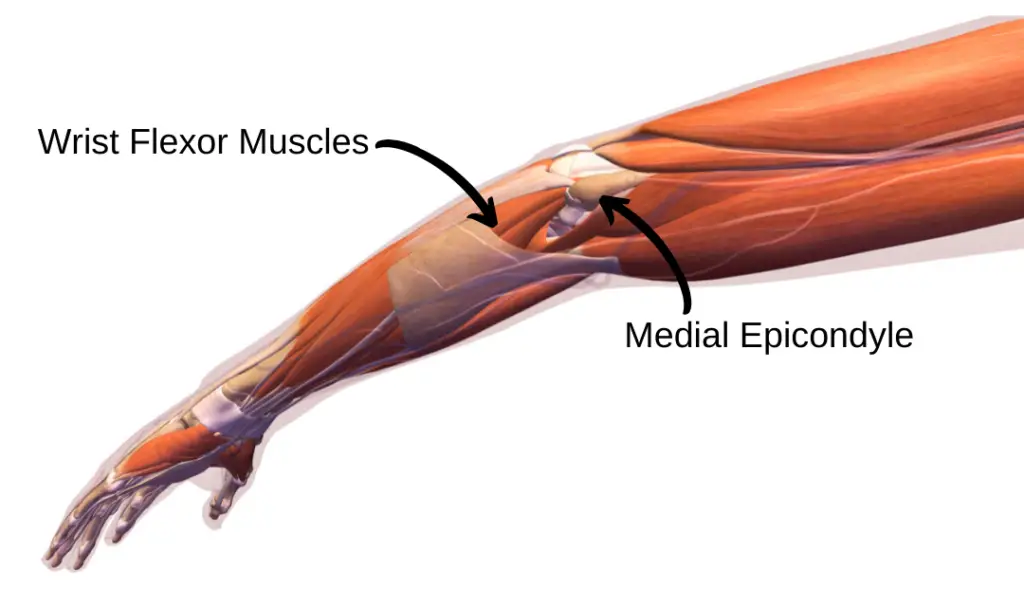
It’s commonly compressed at the cubital tunnel, where the ulnar nerve runs behind the medial epicondyle–the bony bump on the inside of the elbow.

Ever hit your funny bone? It’s actually not a bone – that’s your ulnar nerve!
The ulnar nerve runs close to the surface of your skin on the inside of the elbow, where it’s susceptible to compression and injury. Less often, the ulnar nerve is compressed at Guyon’s canal, on the inside of the wrist near the little finger.
Common Causes
Ulnar nerve irritation is the 2nd most common nerve condition in the arm, behind carpal tunnel syndrome. Ulnar nerve pain at the elbow (cubital tunnel syndrome) occurs after a trauma, like an elbow fracture, or slowly over time.
Elbow pressure and positioning can aggravate the ulnar nerve at the medial elbow. Too much pressure on the elbow or prolonged elbow bending inflames the ulnar nerve.

It’s a common problem for office workers. Especially people who type a lot and spend hours holding the phone up to their ear. Instead, opt for a Bluetooth headset or use the speakerphone to mitigate stress on the elbow.
Sleeping with bent arms and leaning on flexed elbows also aggravate cubital tunnel symptoms.
Ulnar nerve irritation is common in baseball pitchers and long-distance cyclists. In fact, ulnar nerve irritation at the wrist is called handlebar palsy.
Ulnar Nerve Compression Symptoms
Ulnar nerve compression causes hand weakness, difficulty gripping, and muscle loss in the hand. In severe cases, a “claw hand” deformity develops (pictured here).

Extreme symptoms include constant numbness and visible hand muscle loss (atrophy) on the pinky side.
Other Causes
Other conditions mimic cubital tunnel syndrome by producing pain, numbness, or tingling in the elbow and forearm (1).
Cervical Radiculopathy
Cervical radiculopathy involves a pinched nerve in the neck. It sends numbness and tingling into the arm, just like cubital tunnel syndrome.

C8 cervical radiculopathy and cubital tunnel syndrome present with overlapping symptoms like numbness and tingling in the pinky, pain along the inside of the forearm, and hand weakness.
To further complicate diagnosis, “double crush syndrome” can occur, where nerve irritation occurs in the neck and in the arm. So it’s possible to have cervical radiculopathy (a pinched nerve in the neck) and cubital tunnel syndrome (ulnar nerve entrapment at the elbow) simultaneously.
Physicians and physical therapists go to school for almost a decade to understand the intricacies of human anatomy. Anatomy is complex. Understanding the source of pain and developing an effective treatment plan is rarely simple.
Golfer’s Elbow
Golfer’s elbow causes pain on the inside of the elbow. It’s caused by muscle and tendon irritation at the medial elbow, close to the ulnar nerve. However, numbness and tingling are not golfer’s elbow symptoms.
Trigger Point Referral
Trigger points are tight, tender spots in muscles. They can send pain to nearby body regions. Trigger points around the chest and shoulder blade refer pain to the medial forearm and hand.
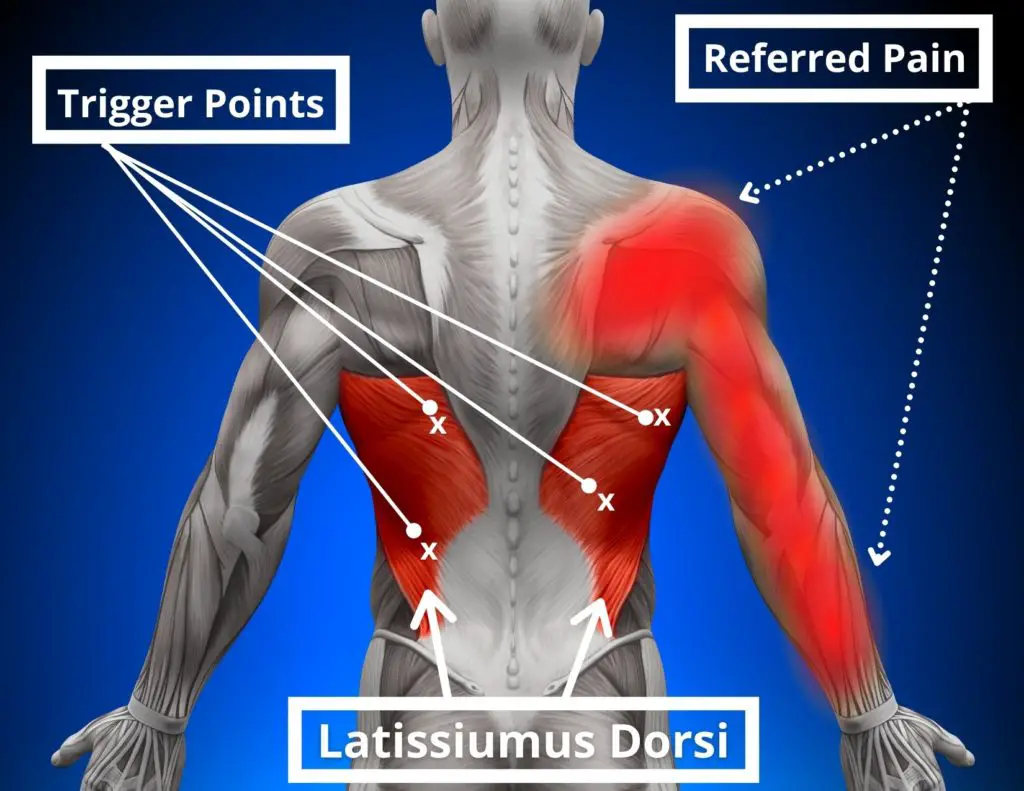
Trigger points in these 3 muscles cause referred pain on the inside of the forearm: the latissimus dorsi, the pectoralis major, and the pectoralis minor.
Thoracic Outlet Syndrome
TOS occurs when nerves and/or arteries are compressed in the neck or shoulder region. Thoracic outlet syndrome causes arm symptoms such as numbness, tingling, weakness and swelling. PT is among the best treatment options, but physical therapy for TOS is much different than treatment for ulnar nerve compression.
Pancoast Tumor
Though quite rare, lung tumors can cause ulnar nerve irritation symptoms.

This problem requires immediate medical attention. Not spinal adjustment, essential oils, CBD cream, or physical therapy exercises.
Don’t Self-Diagnose
Many conditions can cause pain, numbness, and tingling on the inside of your elbow.
Working with a qualified healthcare professional is the best way to rule out serious issues, determine the underlying cause of your symptoms, and recover quickly.
Two Tests
Healthcare professionals use these two tests to assess for ulnar nerve pain.
Tinel’s Test
Tinel’s test isn’t complicated once the correct location is identified. The clinician taps quickly on the ulnar nerve at the cubital tunnel. Symptom reproduction, usually numbness and tingling into the pinky, indicates positive test.
Peep the video to see it in action (and enjoy the sweet British accent)
Ulnar Nerve Tension Test
Clinicians use this test to assess ulnar nerve flexibility. Dramatic differences between arms indicate adverse neural tension (an irritated or tight nerve). Symptom reproduction also indicates ulnar nerve irritation.

Position the arm as shown – Make an “OK” sign and put the “O” over your eye with your hand upside down. The move looks goofy, but it is an actual assessment technique.
It’s normal to feel a stretch at the inside of the elbow. Increase the stretch by elevating the elbow more and bending the neck away from the arm being tested.
6 Ulnar Nerve Exercises
The following interventions are the best nonsurgical treatments to decrease ulnar nerve pain and promote recovery.
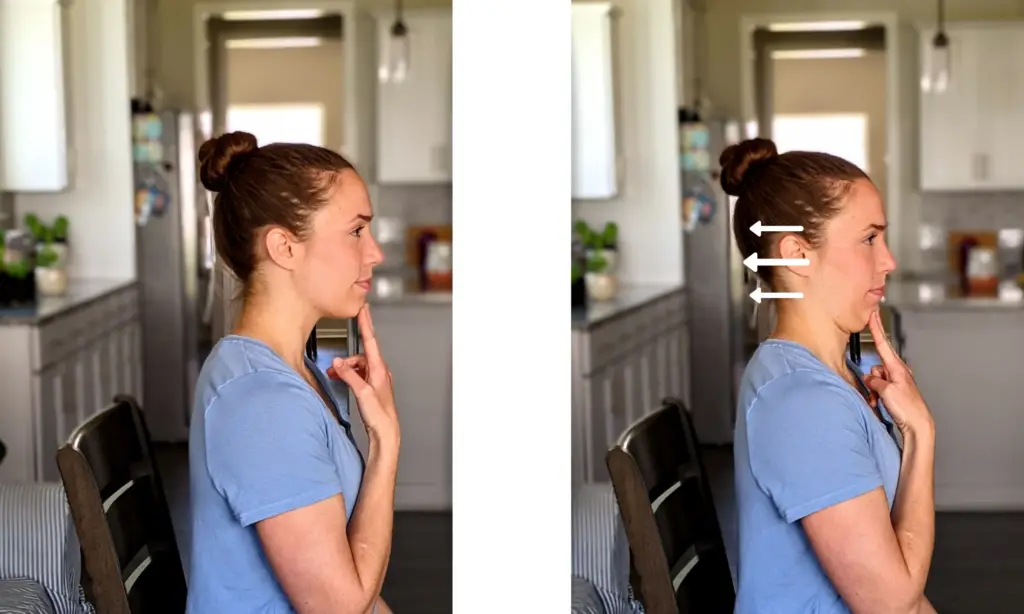
1) Chin Tucks
Also known as cervical retractions, repeated neck movements assess for neck contribution to arm pain. Elbow pain originates from the spine 44% of the time! (2)
Repeated neck motions have zero effect in cases of true ulnar nerve entrapment at the cubital tunnel (elbow) or Guyon’s canal (wrist).
However, chin tucks change symptoms at the elbow, forearm, and hand when there’s referred pain from the neck, cervical radiculopathy, or double crush syndrome.
For more insights on relieving referred neck pain, check out the popular Treat Your Own Neck book which has helped thousands of people gain control over neck pain.
2) Immobilization
For patients with mild symptoms, immobilizing the elbow at night can promote healing and prevent nerve irritation during sleep.

Guidelines recommend bracing the elbow at 45° of flexion for up to 3 months (3). Multiple research studies found the Hely & Weber elbow brace provided effective ulnar nerve compression relief.
3) Ergonomics
For office workers, desk ergonomics can make or break the recovery process.

A protective elbow pad prevents ulnar nerve aggravation during repetitive daily activities, like resting the elbow on your desk.
Also, stay away from these “no-no’s” during the work day to recover faster:
- Avoid excessive gripping
- Limit elbow bending past 90°
- Prevent excessive forearm muscle use
If your workplace ergonomics need help, check out 5 Ways to Sit with Less Pain
In the early stages, ulnar nerve irritation is predictable and worsens with aggravating activities, like frequent elbow bending and wrist compression. It improves with rest and non-aggravating positions.
As ulnar nerve pain progresses, symptoms become more constant and don’t change based on positions and activities. Avoid this stage if possible!
4) Ulnar Nerve Glides
Nerve glides, or neural flossing, gently stretches peripheral nerves to promote healing. It’s an effective technique for sciatic nerve pain and nerve pain in the arms. Neural glides stretch and floss the nerve through its pathway, reducing swelling and restoring blood flow to the nerve (4).
There are two types of nerve mobilization exercises.
Nerve Sliders
Nerve “sliders” floss the nerve back and forth. The nerve slides side to side but doesn’t stretch or lengthen.
It’s like flossing your teeth. The dental floss slides side to side, clearing debris from it’s path. Similarly, nerve sliders smooth the nerve’s path through the arm.
When performed correctly, the patient feels nothing–no stretching, pain, or changes in symptoms during the exercise. Nerve sliders work best when the nerve is easily irritated, like my wife when I leave dirty clothes next to the laundry basket.

First, stretch the ulnar nerve at the hand while slackening at the neck (above). Then, slacken the nerve at hand and lengthen it at the neck (below). Repeat 10-15 times.

Nerve Tensioners
Nerve “tensioners” gently stretch the affected nerve. They work best when the nerve is mildly irritable. Think of lightly stretching a rubber band from both ends. Tensioners are more aggressive than sliders. They can aggravate arms symptoms if done too enthusiastically.

First, stretch the ulnar nerve at the hand and the neck (above). Then, slacken the nerve at both locations (below). Repeat 10-15 times into a gentle stretch.

“No pain, no gain” doesn’t apply here!
5) Wrist Flexor Stretch
Stretching simply for the sake of stretching is probably a waste of time. However, cubital tunnel syndrome creates a protective response where the body instinctively tightens the muscles around the nerve.
With cubital tunnel syndrome, that’s the wrist flexor muscles. Folks with cubital tunnel syndrome often hold the affected elbow in a bent, guarded position.
Straightening the elbow and gently stretching the wrist flexors promotes normal range of motion at the elbow. Like this:
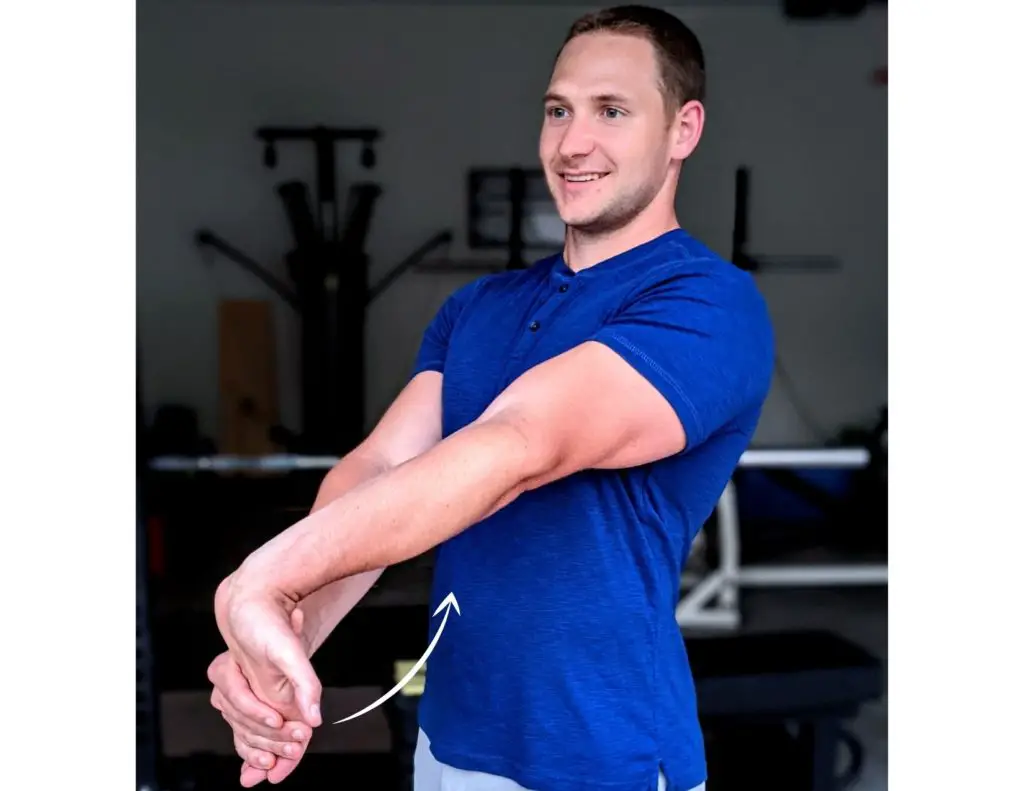
It can even prevent elbow flexion contractures, a condition where the elbow won’t straighten.
6) Ball Squeezes
Ball squeezes strengthen the wrist and forearm muscles. For ulnar nerve injuries, strengthening isn’t the first line of defense. In fact, it can aggravate the ulnar nerve when it’s done too early in the healing process.
Strengthening is indicated once nerve healing begins and sensation returns. Ball squeezes work hand and wrist muscles that become weak with ulnar nerve injury.
Beefing up the weakened muscles is key to regaining hand and arm function. You won’t need your son to open jars for you anymore!
A massage lacrosse ball works best for this exercise.
Other Interventions
Conservative interventions don’t always solve cubital tunnel syndrome. Advanced cases may require surgery to prevent permanent damage to the ulnar nerve.
Severe symptoms include progressive muscle weakness, hand muscle atrophy, permanent sensation changes, and constant pain.
Your doctor may order diagnostic studies such as EMG and nerve conduction studies to assess the extent of nerve damage. Outcomes of these studies guide treatment decision-making.
Overall, surgical outcomes are good – 87% of patients improve after surgery (5). The goal of surgery is to relieve ulnar nerve compression at the inner aspect of the elbow.
The surgeon creates more space for the nerve to travel, and sometimes relocates (transposes) the nerve to reduce pain. Surgeons use several surgical techniques for cubital tunnel syndrome.
Recent research suggests that an open procedure without nerve transposition (in situ) produces the best outcomes and lowest complication risk (6). However, each case is different and surgeons consider many factors when deciding which technique to use.
Conclusion
Ulnar nerve pain causes numbness and tingling in the arm and hand. Non-surgical interventions alleviate many cases of mild to moderate pain. Surgery is the best treatment for severe symptoms.
It’s a good idea to consult with a physical therapist or orthopedic physician, especially if your symptoms worsen or have been going on for a long time. A skilled clinician will determine the exact cause of your symptoms and work with you to develop a customized treatment plan.
For more evidence-based insights you won’t find anywhere else, join the free, fast-growing Facts & Physio Newsletter. Plus, get The Recovery Checklist when you sign up.


6 thoughts on “6 Proven Ulnar Nerve Exercises (Cubital Tunnel Syndrome)”
Just had ulnar decompression surgery on 9/12, interested in helpful recovery exercises.
Thank you
This was very helpful. Will leave a message next time. I’m seeing a neurologist tomorrow.
Glad you found it helpful!
Hi useful, but would be helpful if image was with a right handed person
Very informative!
I’ve gotten both ulnar nerve relocation surgery….going on year 3 in recovering! Never give up right!!
Schwaannoma removed 11/11 : third finger and pinky still weak/unmanageable. Will find a squeezy ball and see how that works.